

Fresh new parents are a on a roller-coaster ride of emotions. Exhausted, happy, uncertain, afraid, panicking. Every decision seems like life and death. I vote for giving them the best evidence-based support we can, while holding the judgement.
After the introduction of modern formula in the mid-20th century, for a time in the developed world, breastfeeding was almost shunned upon. Today the balance is well shifted and breastfeeding is recommended to all mothers who are able to do so. But just how pronounced are the benefits of breastfeeding compared to formula?
I was recently prompted into taking a closer look at the science of breast vs formula feeding once more by a good friend who works as a consultant to mothers with breastfeeding issues, manages breastfeeding forums, gives talks on the topic and also blogs over at Milk and Motherhood. She is the most compassionate and supportive person I know, and she is uncomfortable with the political pressure to strongly promote breastfeeding, while all she would like to do is to allow women to fulfil their personal dreams of motherhood, whatever they might be. I find this to be a great sentiment, especially in the light of the available evidence: it is in the best interest of mothers and their babies that we are allowed to use both methods of infant feeding. Depending on the situation, breast and bottle-feeding both have their own set of benefits. Babies as well as mothers are worse off if the access to either of the options is culturally sabotaged.
The benefits in the developing world are clear
In the developing world lack of access to good drinking water, unhygienic conditions, and the cost of formula are really decisive factors that dramatically shift the situation in favour of breastfeeding. UNICEF estimates that a formula-fed child living in disease-ridden and unhygienic conditions is between 6 and 25 times more likely to die of diarrhea and four times more likely to die of pneumonia than a breastfed child. In the light of these statistics, it is clear why the World Health Organisation generally recommends breastfeeding. They recommend exclusive breastfeeding for 6 months, and encourage continuing partial breastfeeding for two years or more. These guidelines are aimed at preventing malnutrition in children, which is still a serious problem globally:
Complementary feeding typically covers the period from six to 24 months of age, and is a very vulnerable period. It is the time when malnutrition starts in many infants, contributing significantly to the high prevalence of malnutrition in children under five years of age worldwide.
In these conditions it is important for the protection of the newborn to breastfeed, and wherever accessible, to get all appropriate vaccines available. As an example, the rotavirus vaccine, prevents two thousand infant diarrhea-related deaths every year after its recent introduction in Mexico and Brazil.
To understand some of the more inflammatory attitudes toward formula feeding better, it helps to learn more about how the topic of breastfeeding has been politicised in the past by unethical practices in the marketing of formula to new mothers in the developing world.
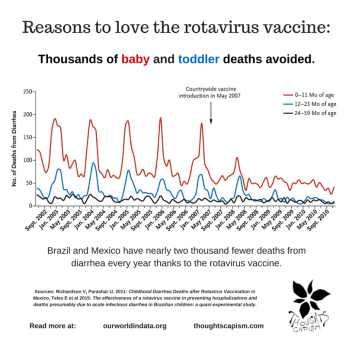
Breastfeeding and the rotavirus vaccine help prevent diarrhea-related deaths in the developing world.
International Baby Food Action Network (IBFAN) claims that Nestlé distributed free formula samples to hospitals and maternity wards in Africa the 1970s, when interest in formula in the west was diminishing. When the families in Africa would leave the hospital, the formula would no longer be free, but generous supplementation would have interfered with lactation, and the families would need to continue buying the formula – this in above-mentioned disease-ridden and unhygienic conditions, and among people living in poverty. You can read much more about the story, law suits, and the since-implemented international code of conduct for the marketing of formula on the Wikipedia page for Nestlé boycott.
But what about the developed world?
The health benefits of breastfeeding depend on the situation, and in the west, where the situation of mothers and babies is otherwise easier, the benefits of breastfeeding are also significantly smaller. There parents have the economy and necessary hygienics needed to provide their children perfectly safe and adequate nutrition in the form of formula. But considering the clear benefits of breastfeeding for children in the developing world, some find little reason to defend the mother’s choice in the matter in the developed world, and see it merely as a sign of privilege. I think the larger issue here is that we should treat all mothers well, and in the absence of clear and significant health concerns, we should not unnecessarily judge others’ parenting decisions. We should carefully evaluate the evidence before condemning one choice over the other.
So, how strongly should women be encouraged to breastfeed? The recommendations of the medical world should be based on the best possible evidence. But, as expressed in science speak: differences in maternal education, hereditary factors, and family income may introduce a bias in study results. Much of breastfeeding research suffers from specific confounding socioeconomic factors, namely those known as ‘mothers’.

Reading to children early on has many benefits for their development
That is to say, mothers who are better off, better educated, and have higher IQs are among the ones who more often choose to and have the possibility to breastfeed. But they are also a group more likely to make health-conscious parenting and life-style choices, like supporting a varied diet, not smoking, including regular exercise, reading to their children, etc, and thus more likely to have children with better health and (hereditarily and thanks to stimulating environment) higher IQs.
To give an idea about the magnitude of studies on this topic which have not controlled for the socio-economic factors of the parents, you can read this review from 2007:
Forty-three primary studies on infant health outcomes, 43 primary studies on maternal health outcomes, and 29 systematic reviews or meta-analyses that covered approximately 400 individual studies were included in this review. […]
Because almost all the data in this review were gathered from observational studies, one should not infer causality based on these findings. Also, there is a wide range of quality of the body of evidence across different health outcomes. For future studies, clear subject selection criteria and definition of “exclusive breastfeeding,” reliable collection of feeding data, controlling for important confounders including child-specific factors, and blinded assessment of the outcome measures will help. Sibling analysis provides a method to control for hereditary and household factors that are important in certain outcomes.
A randomized breastfeeding trial: benefits are small
The above review mentions that there are some studies that have carefully controlled for this mother-factor: sibling studies – studies that look at the situations where one child was breastfed and the other was not. But there is also one rare case of a randomised study from Belarus, known as the PROBIT trial, conducted in 1996, where one group had higher rates of breastfeeding after a breastfeeding recommendation, attributing less of the breastfeeding choice to the parents’ socioeconomic background.
The study included 1700 mothers all in all, and the group which received the breastfeeding recommendation intervention had following breastfeeding rates:
- exclusive breastfeeding at 3 and 6 months age,respectively, 43.3 and 7.6 %.
- The corresponding rates in the control group were only 6.4 and 0.6 %.
- At the 12 month-point, 19.7 % of the mothers in the intervention-group were still breastfeeding their babies to some degree.
- The rate in the control group was only 11.4 %.
The intervention, in other words, did have an indisputable effect on the breastfeeding rate, and while it is possible that the recommendation had more or less impact on mothers of a higher or lower socio-economic status, this still allowed the researchers to compare hundreds of mothers to each other with more comparable background factors than in simply observational studies, since the great majority of mothers in the control group chose not to breastfeed. And the study’s findings?
- The rate of gastrointestinal tract infections for the intervention group was 9.1%, whereas the rate in the control group was 13.2%.
- Atopic eczema was present in 3.3% of the intervention group babies, and 6.3% of the babies in the control group.
- They found no significant reduction in respiratory tract infection (intervention group, 39.2%; control group, 39.4%).
- Same was true for respiratory infections, ear infections, croup, wheezing and infant mortality.
So that was it. The group with significantly more breastfed babies had slightly lower rates of gastrointestinal infections and eczema. Avoiding such conditions during the first year is certainly a boon for any mother, and it’s a benefit which is good for mothers to know about. However, it is hardly something that would give us reason to ostracise mothers less inclined to breastfeed.
An article at fivethirtyeight, Everybody calm down about breastfeeding, does a great job of summarising a lot of breastfeeding research. They lay out many common claims – and the lack of support for them – from further studies based on the rigorous randomised PROBIT trial, like one about obesity and metabolic effects. Fivethirtyeight notes:
Many sources (for example, that poster in my midwife’s office) go further and claim that breastfeeding has health benefits for the child in the long term — lower obesity risk, better blood pressure and so on. And on top of this, there are the claimed benefits on behaviors — less hyperactivity, fewer behavior problems, more maternal attachment, etc.
Here, the evidence is not mixed. It rejects these claims across the board.
The PROBIT randomized trial is again the best source. The researchers analyzed the impacts of breastfeeding on allergies and asthma; on cavities; and on height, blood pressure, weight and various measures of obesity. They found no evidence of nursing’s impacts on any of these outcomes. They also found no evidence of impacts on child behavior issues, emotional problems, peer issues, hyperactivity or maternal-child connection.
Sibling studies confirm: mothers are the biggest factor

There are many great things about siblings. For science too.
Looking at siblings, where one has been breastfed and the other not, is the best way to control for the parents’ socioeconomic status. These studies largely continue in the same tune as the PROBIT trial, with even less support for significant effects from breastfeeding over formula in full term babies in the developed world. A US 2014 study: Is breast truly best? Estimating the effects of breastfeeding on long-term child health and wellbeing in the United States using sibling comparisons, found the following:
Results from standard multiple regression models suggest that children aged 4 to 14 who were breast- as opposed to bottle-fed did significantly better on 10 of the 11 outcomes studied. Once we restrict analyses to siblings and incorporate within-family fixed effects, estimates of the association between breastfeeding and all but one indicator of child health and wellbeing dramatically decrease and fail to maintain statistical significance. Our results suggest that much of the beneficial long-term effects typically attributed to breastfeeding, per se, may primarily be due to selection pressures into infant feeding practices along key demographic characteristics such as race and socioeconomic status.
What was that one factor which remained significant, you might wonder? The outlier was asthma, but it was found to be associated more with breastfeeding than with bottle-feeding. You can read more about the trial in this Ohio University press release: Breast-feeding Benefits Appear to be Overstated, According to Study of Siblings.
An earlier study from the UK in 2006, which included a sibling analysis, had similar findings: Effect of breast feeding on intelligence in children: prospective study, sibling pairs analysis, and meta-analysis. They report no difference in intelligence in children based on feeding choice, pointing instead at maternal intelligence as the significant predictive factor:
Before adjustment, breast feeding was associated with an increase of around 4 points in mental ability. Adjustment for maternal intelligence accounted for most of this effect. When fully adjusted for a range of relevant confounders, the effect was small (0.52) and non-significant (95% confidence interval -0.19 to 1.23). The results of the sibling comparisons and meta-analysis corroborated these findings.
CONCLUSIONS:
Breast feeding has little or no effect on intelligence in children. While breast feeding has many advantages for the child and mother, enhancement of the child’s intelligence is unlikely to be among them.
There is, however, a special case even in the developed world, where breastfeeding is a more significant health factor: pre-term infants.
Pre-term infants clearly benefit from breastfeeding
An important area highlighted in the American Association of Pediatrics 2005 overview of breastfeeding concludes that there are benefits of breastfeeding for infants born before term, whose digestive systems are not yet well developed, and pass through a lot more of the antibodies present in mother’s milk, than do even the guts of babies a few weeks or months old. These benefits for pre-term infants are profound:
human milk-fed premature infants receive significant benefits with respect to host protection and improved developmental outcomes compared with formula-fed premature infants. […]
Research in developed and developing countries of the world, including middle-class populations in developed countries, provides strong evidence that human milk feeding decreases the incidence and/or severity of a wide range of infectious diseases including bacterial meningitis, bacteremia, diarrhea, respiratory tract infection, necrotizing enterocolitis, otitis media, urinary tract infection, and late-onset sepsis in preterm infants. In addition, postneonatal infant mortality rates in the United States are reduced by 21% in breastfed infants.
There is yet another group of people who may enjoy benefits of breastfeeding, namely: the mothers.
Mothers can benefit from breastfeeding – as well as from having the choice to formula feed
There are many documented upsides that mothers may enjoy thanks to breastfeeding, anything from faster birth recovery to the repressive effect on fertility, helping mothers avoid becoming pregnant in too rapid a succession, as well as reduction in breast cancer risk, and a potential for weight loss. The American Association of Pediatrics 2005 overview concludes it as follows:
Important health benefits of breastfeeding and lactation are also described for mothers. The benefits include decreased postpartum bleeding and more rapid uterine involution attributable to increased concentrations of oxytocin, decreased menstrual blood loss and increased child spacing attributable to lactational amenorrhea, earlier return to prepregnancy weight, decreased risk of breast cancer, decreased risk of ovarian cancer, and possibly decreased risk of hip fractures and osteoporosis in the postmenopausal period.

Mother’s mental and physical well-being is very important for the baby’s sake, too.
Mother’s well-being should not be ignored, either, among the factors influencing babies’ development. Judgement over mother’s choice to either breast or bottle-feed, however, is as likely to be helpful for her mental and physical well-being as it would be to express judgement about her getting enough sleep or moments to relax, or finding the time to have regular balanced meals and do exercise.
As pointed out in the piece UNICEF Breastfeeding Recommendations Paint With Too Broad A Brush over at the American Council on Science and Health:
Breastfeeding went from being controversial in public settings to being a culture war against working mothers. It’s not like smoking or exercise, where the weight of evidence is clearly on the side of giving up the former and taking up the latter.
It is important to realise, that mother’s circumstances, anything from medical (such as medications, infectious diseases) and mental health (like post-partum depression) issues, to societal circumstances (needing to return to work) and personal preferences (wish to be able to spend time away from childcare, difficulty or inability to use a breast pump), are also important factors that weigh in on the feeding choice and can influence the baby’s health and development. In the developed world, where the evidence-based benefits of breastfeeding are small, a mother’s happiness is easily a larger factor for the child’s overall wellbeing than feeding source, whereas having a choice between feeding options can be highly beneficial for the mother and her personal life situation.
A mother who has had a good night’s sleep, while the father has taken care of night feeds, for instance, is a mother who is much more likely to be active, happy, and communicative with her baby during the day time. A sleep-deprived mother who, furthermore, is guilt ridden over her continued failure to breastfeed is also much more likely to suffer graver effects from the already difficult time of hormonal wasteland following birth, and more at risk for having a post-partum depression. An article in Slate from 2009, The case against breastfeeding, offers another long look at the science and culture wars around infant feeding, and gives a good idea about the ambivalence towards breastfeeding which many mothers may experience.
It is worth noting that when people in the west say ‘breast is best’, their main focus is rarely the mothers themselves, or the babies in the developing world: it’s the health of normal, full-term babies in the developed world. Many go as far as to claim that choosing formula would put these babies at risk.
Psychological pressure heaviest on the group with least evidence of benefits
So there are good grounds to recommend breastfeeding over formula for: 1) babies in the developing world; 2) for pre-term babies; as well as 3) for mothers themselves. Babies in the developed world, who are born full-term, however, seem to be in different situation, and have a much decreased risk from most of the conditions listed for pre-term infants or children in the developing world, and according to the best evidence, they are not really better or worse off whether breastfed or not.
These three aforementioned groups are rarely the target of the very breastfeeding-focused, and even formula shaming, culture that has emerged in many places, commonly among groups of well-off parents in the developed world. Many maintain that it is imperative to get more mothers to breastfeed their babies. Many hospitals and health care professionals, like those involved in the Baby Friendly Hospital Initiative, go to great lengths to attain higher breastfeeding rates. As one MD writes in the Salon:
It starts in some hospitals, where the clear message is that choosing to formula-feed one’s infant is baby “unfriendly.” It comes from lactation support professionals who are too assertive in stating their viewpoint when meeting new mothers on postpartum wards. And of course, it comes from other mothers.
The message communicated is that all women can and should breast-feed their babies, and that it is innately selfish and harmful to choose otherwise.
A comment from the article in fivethirtyeight sums the situation well:
It shouldn’t come as a surprise, then, that many women who struggle to breastfeed (or just find it annoying and want to quit) feel ashamed and sad that they are not giving their children the “best” start in life. It wouldn’t be great to make women feel this way even if all the purported benefits of breastfeeding were real. It’s even worse because the truth is that the vast majority of these claims are way overblown.
The expectation that everyone will be able to breastfeed if they just try, and the blown up focus on suggested benefits can backfire, when mothers who simply are not able to succeed with breastfeeding are left with a terrible feeling of guilt over their failure. The story of my friend Johanna is one of these stories, and it still easily brings me to tears.
Breastfeeding focus in overdrive?
Quite recently researchers have raised caution over too breastfeeding-focused practices, in the viewpoint piece published in Journal of American Medical Association: Unintended Consequences of Current Breastfeeding Initiatives. While breastfeeding is a great way to feed a baby, the gist of the evidence supports the view that choice of feeding method should not be considered an all-important one among parenting decisions. The paper warns that:
there is now emerging evidence that full compliance with the [Ten Steps to Successful Breastfeeding of the Baby-Friendly Hospital] initiative may inadvertently be promoting potentially hazardous practices and/or having counterproductive outcomes.
Covered also in a piece by Elissa Strauss in Slate, Baby-Friendly Hospitals Can, Paradoxically, Be Unsafe for Newborns. She reports that the paper authors:
question whether supplementation with formula should really be banned, as there is no hard evidence linking early formula use to a decreased likelihood of breastfeeding further down the line. In fact, one study suggests that early formula use might help increase breastfeeding rates by reducing stress among new moms while they wait for their milk to come in.
I found this study reference especially interesting, as I had always simply assumed that any supplementation would interfere with breastfeeding success. Yet in this three year old study, those mothers who were allowed to supplement with small amounts of formula with a syringe in the early days after birth were found to succeed better with breastfeeding. There were only 40 mothers in the study, and it would be interesting to see larger studies on the topic, but its results are promising. Here’s a news piece about the study, Early formula use helps some mothers breastfeed longer:
The study enrolled 40 full-term newborns between 24-48 hours old who had lost more than 5 percent of their birth weight. […]
After three months, 79 percent of the babies in the study who received early limited formula in the first days of life were still breastfeeding, compared with 42 percent of the babies who did not receive early limited formula. Additionally, 95 percent of the babies who received limited formula in the first few days were breastfeeding to some extent at three months, compared with 68 percent of the babies who did not receive early limited formula.
Should mothers be scared of formula?
The above cited study certainly casts some doubt on the way some groups, like the Adademy Breastfeeding Medicine (ABM), have insisted that campaigns should expressly inform future mothers about the risks of formula. Their arguments rely largely on the results from studies where the mother’s socioeconomic background actually accounts for the vast majority of the differences, not breastfeeding per se, as outlined here earlier. ABM also puts forward an argument of a possible protective effect from breastfeeding against childhood leukemia. A look at one recent review does suggest that breastfeeding could reduce its incidence by 14-19 %.
 If this kind of protective effect exists, we should certainly not ignore it. To understand the topic better, let’s consider the background. Because the incidence of childhood leukemia is relatively low, it is not the easiest topic to study epidemiologically. According to the NIH’s National Cancer Institute there are approximately 72 cases of leukemia per 1 million children under five. Considering this, it would have been hard to find confirmation for such an effect from sibling studies – there are simply too few cases of leukemia to get a proper signal with a sample size smaller than in the hundreds of thousands. Otherwise randomized or sibling studies would still be the best type of studies to rule out that hereditary and other household factors are not at play.
If this kind of protective effect exists, we should certainly not ignore it. To understand the topic better, let’s consider the background. Because the incidence of childhood leukemia is relatively low, it is not the easiest topic to study epidemiologically. According to the NIH’s National Cancer Institute there are approximately 72 cases of leukemia per 1 million children under five. Considering this, it would have been hard to find confirmation for such an effect from sibling studies – there are simply too few cases of leukemia to get a proper signal with a sample size smaller than in the hundreds of thousands. Otherwise randomized or sibling studies would still be the best type of studies to rule out that hereditary and other household factors are not at play.
But let’s say for the sake of the argument that this observed decrease in leukemia rate would not be a result from confounding hereditary or socioeconomic factors, but of breastfeeding. It would imply that on average the rate of childhood leukemia could be reduced from 72 to between 58 and 62 cases per one million children under five. Any reduction in childhood cancers is tremendous, but for us to be sure that the effect is real it would be better if the results could be confirmed by sibling data, or be supported by finding a probable mechanism of action, or other methods better aimed at elucidating the causal relationship between these factors.
Some of the studies that observed the effect again readily acknowledge their possible biases:
Alternative explanations must be considered. The observed inverse association with breast-feeding may reflect a potential selection bias due to the source of control subjects (random-digit-dialing) and different participation rates among control and case subjects. The difference between case and control subjects in maternal education and family income may also suggest the possibility of selection bias (27).
A Review of case-control studies related to breastfeeding and reduced risk of childhood leukemia from 2005 has earlier concluded as follows:
There are few high-quality studies that examine the potential for a protective effect of breastfeeding for childhood leukemia. Furthermore, the few studies that exist disagree regarding the association.
The American Cancer Society for instance makes no mention of breastfeeding in their article on risk factors for acute childhood leukemia, instead they list better confirmed factors such as inherited syndromes (like Down’s), several inherited immune system problems, chemotherapy, benzene, possibly other chemical exposures, and immune system suppression (transplant patients). Scientists believe that two genetic changes are needed to cause the disease and that one occurs before a child is born (page 21 in the NIH Cancer report). It looks like there are plenty of potential hereditary and environmental confounding factors at play here.
So, the question is: if such a protective effect of breastfeeding would exist, would it be large enough to merit scaring and shaming millions of mothers for the sake of choosing formula? At the level of evidence we have at present, I would argue that scaring people about formula seems ill-advised. Infant feeding is a multi-faceted matter, and there is also convincing evidence that a strong stance against formula comes with its own set of risks. Let’s look at that next.
Making formula seem risky, is risky and unhelpful
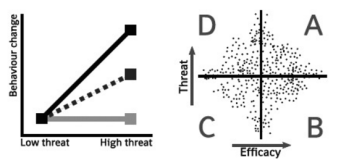
Left: effect of fear appeals. Black line for groups with high efficacy, grey under low efficacy, and the dotted when efficacy levels are disregarded. Right: distribution of threat and efficacy associated to a random sample of behaviour-population combinations.
Even the researcher at the ABM, who earlier promoted the tactic of speaking about risks of formula, rather than benefits of breastfeeding, has had some second thoughts about her risk based language: studies examining the effects of health recommendations with threatening messages have noted that they may not work as well as positive encouragement and providing information about benefits. Positively focused approach is recommended even in a topic as clearly risky as smoking during pregnancy, especially when it comes to mothers from lower socio-economic backgrounds with lower sense of agency, or efficacy. In other words, risk-based messages work least well with the very mothers who are the main target of breastfeeding campaigns.
This campaigning of ‘formula as a risky choice’ -approach becomes even trickier when breastfeeding campaigns succeed in convincing mothers that even one bottle of formula will somehow harm their child. Not only can it be psychologically devastating for the mother who fails to breastfeed despite her best efforts, negatively influencing her mental health in a vulnerable time, but it may also make people overlook some important health risks during the infant’s first week of life, that could actually be remedied by supplementation with small amounts of formula.
The Fed Is Best foundation, formed by physician Christie del Castillo-Hegyi and NICU nurse and lactation consultant Jody Segrave-Daly, on the other hand works to counteract too breastfeeding focused campaigns, and wants to support mothers whether they choose to breast- or bottle feed. In her personal letter to doctors and parents, del Castillo-Hegyi, who has worked in newborn brain injury research, highlights an issue I had not really stopped to consider before – that babies, whose mothers don’t produce enough milk sufficiently quickly after birth, are at risk from low blood sugar levels, or hypoglycemia. She also points out that 10-18 % of exclusively breastfed babies in the US are at risk for starvation induced jaundice. This lack of nutrition could give rise to grave consequences for the baby’s brain development if not addressed properly, but it can be addressed with very simple means: by supplying small amounts of donor milk or formula until the mother’s own milk is sufficient. Del Castillo-Hegyi writes:
In a study of 280 mother-baby dyads, 22% of motivated mothers intending to exclusively breastfeed who received close lactation support experienced delayed onset of copious milk production, or lactogenesis II, which put her child at 7-fold increased risk of excessive weight loss greater than 10%. This means more than 1 in 5 newborns are at risk of starvation-related complications if exclusively breastfed from birth. In another study, it has been found that 10% of well-monitored exclusively breastfed babies undergoing the Baby-Friendly Hospital Initiative protocol develop hypoglycemia of less the 40 mg/dL within the first 48 hours. This incidence was even higher in babies born to first-time mothers as 23% developed hypoglycemia.
This does not mean that breastfeeding would not have benefits – as summarised earlier, it does, although the benefits are much smaller than commonly thought for normal full-term babies in the developed world – but these observations do point out that an absolute focus on exclusive breastfeeding does not always take into consideration the best interests of the infant during the firsts days of life.
Meanwhile, absolute avoidance of formula is exactly what some lactation consults lecture: they imply that just one bottle of formula is harmful. Setting aside the lack of reliable evidence to support this position, it actually means that they are knowingly setting up between 22 – 44 % of mothers (those who experience late onset of milk production, studies here and here) to believe they have failed, and to think that they are now forced to ‘harm’ their child.
Journalist Kavin Senapathy does a great job interviewing doctor del Castillo-Hegyi from Fed is best. In her piece she brings up several studies whose results go counter to common beliefs about breastfeeding – like the one I referenced about supplementing, which found that small amounts of supplement in the early days can actually help mothers succeed with breastfeeding in the long term. Del Castillo-Hegyi also pointed to one which surprised me, as it questions wet diapers as a signal of sufficient feeding:
…a study in the Journal of Human Lactation on newborn wet diaper counts showed that even babies who developed abnormal weight loss of greater than 10% were still able to produce wet and soiled diapers. “Weighing the baby and the amount of milk transferred to the baby is the only objective measure of adequate feeding,” she says.
But surely breastfeeding has evolved to fit the infant’s needs?
Many people feel that breastfeeding, being the natural way of taking care of our infants, must work well enough on its own, and no interference with this process should be necessary. Yet many forget that the way we have evolved to this point does not come with any individual guarantees of success – from a biological point of view, evolution of any mechanism which allows for a significant enough portion of the individuals to survive, is sufficient for the species to continue inhabiting its place in the ecosystem. When humans developed greater mental capacities, for instance, it was a great evolutive advantage, and the following higher failure rate of giving birth to babies with larger heads was not a large enough disadvantage to counteract that trend.
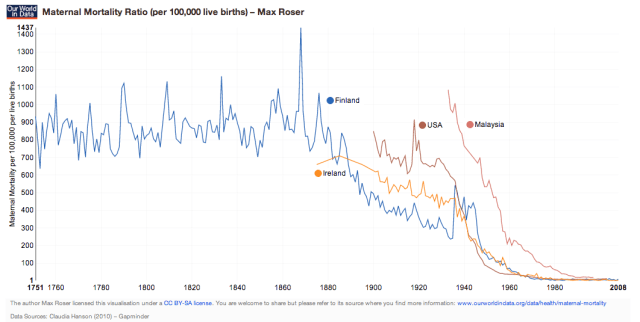
Not only the mortality of children but also the mortality of their mothers decreased dramatically in the last two decennia. A hundred years ago a woman was more than 70 times more likely to die while giving birth. Source: Our World In Data, Global Health.
Same applies to lactation success: from a natural point of view, that a majority of mothers succeed with breastfeeding is ‘good enough’. But from a humane perspective, every baby who suffers or dies is a needless victim, when we can use our natural resourcefulness and cognitive abilities to our advantage and develop other ways of helping those mothers and babies who are not as lucky.
There used to be little we could do for women in labour, and giving birth remained a hazardous business for a long time (see the graph above). But as far back as the times of ancient Egypt it was commonplace to help mothers who struggled to feed their infants either with wet nurse services or by offering animal milk substitutes. In modern times, we can do much more for the health of mothers and babies with the help of things like medicines, surgery, vaccinations, neonatal intensive care units, and yes, formula.
All these factors, as well as improved food provisions globally, are what we have to thank for for the radical change in infant mortality rates within even the past 60 years. You can take a look at the interactive map depicting the fall of neonatal mortality rates all over the worl over at Our World In Data.
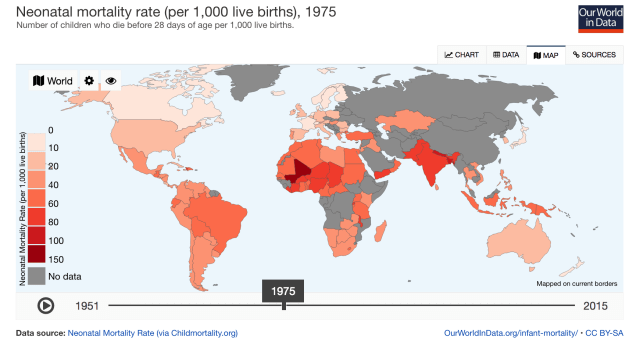
Check the interactive graphic to follow the decreases in infant mortality over at Our World In Data.
Del Castillo-Hegyi elaborates on this point in his interview with Kavin Senapathy:
Del Castillo-Hegyi explains that one “logical fallacy of breastfeeding education is that humans have evolved perfectly and therefore nature protects our babies.” She stresses that this is misguided, and that historically, babies died when mothers who failed to lactate couldn’t find a wet nurse or another source of milk. “Luckily, humans developed an alternative that allowed the least-fed to survive, an alternative that is being made less available to mothers who are made to feel like failures for using it”
Support of neither, breast- or bottle feeding, should happen at the cost of the other
Providing a baby with a safe and adequate source of nutrition is the number one responsibility of new parents. Dogmatism in a topic where the evidence does not give us one simple right or wrong answer only works to add to the negative, stressful aspects of parenting. Let’s instead aim at giving parents emotional support and improving general understanding of the nuances of infant feeding research.

Breastfeeding in the public is protected by law in most western countries, but it may not be as well socially accepted everywhere. We Finns, however, don’t really think twice about it.
It is a good thing help normalise breastfeeding, working toward the goal that mothers breastfeeding out in the public can do so without judgement. We should give women adequate support and knowledge about ways which help with lactation success, and additional ways that can help when the mother wishes to breastfeed but cannot do so exclusively – say like the supplemental nursing system. As the excellent fivethirtyeight article puts it:
Many women find breastfeeding to be an enjoyable way to bond with their babies. There is certainly no evidence that breastfeeding is any worse for a baby than formula. And maybe there are some early-life benefits in terms of digestion and rashes, which you may or may not think are important. But what the evidence says is that the popular perception that breast milk is some kind of magical substance that will lead your child to be healthy and brilliant is simply not correct.
Let’s also give our support to mothers who choose to bottle feed, and work to dispel the stigma that some wish to attach to that choice. Formula feeding, in the fortunate conditions of the developed world, is a great choice for providing for the baby. Nothing more, nothing less. It’s great that we have this option, and I hope that the choice will soon be safely available for every mother, all over the world.
It should not be too difficult to find a way of keeping both options open, arriving at a win-win situation for the mental and physical health of both, the parents and their babies. I think the Slate article expressed it well:
it’s possible to encourage breastfeeding without making breastfeeding the sole focus of the maternity ward—an objective that can all too easily come at the expense of a woman’s autonomy and an infant’s health. What families need is hospital-based breastfeeding support that is responsive to the physical and psychological needs of the mom and doesn’t prioritize feeding over other aspects of an infant’s health.
Another thing I hope we can help promote all over the world is an atmosphere of empathy and support when it comes to the challenging endeavour of parenting. Wherever possible, it is important to try be accepting of our differences, and reserve strongly expressed recommendations for situations where the evidence does unequivocally point toward one choice above others – and even then, I hope we can learn to communicate respectfully, treating each other well, in a way that makes the world a kinder place.
In the words of my friend over at Milk and Motherhood:
I want to live in a world where nobody feels uncomfortable when they see a woman feeding her child, in whichever way is working for them.
![]()
You can go here for more of my articles on the topic of: Vaccines and Health. If you would like to ask a question or have a discussion in the comments below, you are very welcome, but please take note of my Commenting policy. In a nutshell:
- Be respectful.
- Back up your claims with evidence.


Pingback: On Breastfeeding - PostpartumParent.com ~ PostpartumPTSD.com
Thank you for such a thorough piece. My son is now 20 months old, but his first few days of life were a nightmare. He struggled to latch, I struggled to produce milk, but our “baby-friendly” hospital told us to keep trying and not to supplement when we went home. He was readmitted to the same hospital on day 3 for dehydration, excessive weight loss, and an inability to coordinate his suck-swallow-breathe reflex with a bottle. All through our struggles, I felt that the only thing that mattered to any nurse, doctor, lactation consultant, any medical professional was that I breastfed as much as possible. We stopped at 2.5 months and used formula until he turned 1. He was healthy, grew like a weed, and loves a huge variety of solid food, but I couldn’t stop feeling like I’d failed him. That is, until I learned how trivial the benefits of breastfeeding him would have been. And that I most likely have insufficient glandular tissue, based on the shape and lack of pre- and postpartum growth in my breasts. I learned all this on my own from articles like yours and the Skeptical Ob’s, well after my son’s first birthday. So thank you, again, for calling for an end to this ridiculous “war” on infant feeding. It helps those of us who nature failed feel less like failed mamas.
LikeLiked by 1 person
Breastfeeding has maternal benefits: lowers risk of breast cancer, cardiovascular disease, metabolic syndrome.
That study of siblings cited went into great detail about the outcomes, but breastfeeding was defined as either yes or no. This makes the results useless, because a mother who breastfed for 2 weeks would be defined as breastfeeding. Labbok and Krasovec in 1990 developed a way of defining breastfeeding: from full through partial (high, medium or low) and token.
Raisler et al. did a beautiful study, tracking women as they changed feeding categories, to conclude that the benefits of breastfeeding are dose related, no matter what is the mother’s socioeconomic status.
No war. Our nation needs paid maternity leave, and everybody else to get on board with breastfeeding, because most women do want to give it a try. We can’t tell women about the health risks of not breastfeeding, without giving them the acceptance, appreciation, encouragement, and practical advice to be able to breastfeed.
The most important thing is for a mother to love her baby. That is paramount. At the same time, as a healthcare professional, I wish every baby could be breastfed and am working hard to open doors to make it easier for mothers.
Some women can’t deliver vaginally and have feelings about that. Some women can’t breastfeed and have feelings about that. Those variations are no reason to ignore basic physiology, when almost all women start making milk in pregnancy under the influence of placental hormones, and have their milk volume increase once the placenta is delivered. No one can choose to avoid those events; they are part of our biologic template, our operating system. The challenge is to create a world where women won’t be throwing their milk away, but giving it to the baby instead.
Research doesn’t have to be a RCT to have results that are reliable and valid.
What about the impact on ecology and the environment of trying to make human milk in a factory, and packaging it and shipping it? Our globe can’t afford that any more.
I am looking for the studies that show the health benefits of formula feeding. In 40+ years, I’ve never found any. Some companies have gotten in trouble for making false claims.
Enough war though, I am sick of that too!
LikeLiked by 1 person
Nikki I could kiss you. The definition of “breastfeeding” in this research is not agreed upon and as you said being “breastfed” is does related when it comes to health outcomes. These studies tell us nothing until they follow breastfed children who are actually EBF for 6 months with continued BF for at least 2 years, compared with formula fed children.
LikeLike
Hello Meg!
Thanks for your interest in my piece. I am not sure what you mean with definition of “breastfeeding”. I am sure these mothers did breastfeed, not “breastfeed”…? As you can read from my long reply to Nikki, the study actually does look directly at whether duration of breastfeeding affects any of the variables studied (it didn’t, and there was even a reverse effect in obesity and BMI).
As you can read from my long reply to Nikki, the study actually does look directly at whether duration of breastfeeding affects any of the variables studied (it didn’t, and there was even a reverse effect in obesity and BMI).
These several studies which included thousands of mothers and babies do look at real life scenarios of breastfeeding across socioeconomic backgrounds. If there is an impact of breastfeeding, then we should indeed see the effect in these large, most well controlled studies. Shorter durations could show smaller effects, and longer durations larger effects, but we don’t see that. Apart from the two single small effects seen in the PROBIT trial, no such effects are found. We could potentially see that a certain amount of breastfeeding is ‘enough’ and more does not yield benefits even in the slight differences in the rates of rashes and diarhhea. There is however no logical reason for a mysterious ‘threshold effect’ that would first come in effect with babies who are breastfed for more than two years.
Please let me know if there is something else you would like to talk about concerning the definitions of breastfeeding or the types of studies that exist, and what they can tell us. Thanks for stopping by!
Best regards,
Iida/Thoughtscapism
LikeLike
Hello Nikki!
Thanks for your thoughtful comment with nods to other studies. I am a bit concerned, however, with your comment about the sibling studies, which is not correct:
“That study of siblings cited went into great detail about the outcomes, but breastfeeding was defined as either yes or no. This makes the results useless, because a mother who breastfed for 2 weeks would be defined as breastfeeding. ”
If you do read the study, you notice directly that this claim is false. They explicitly note two ways in which they report and analyse breastfeeding data: if the child was breastfed at all AND the duration of breastfeeding measured in weeks, by surveying the mothers on the date of termination of breastfeeding. That survey took place within the first three years of life in order to make sure the estimates were accurate.
They analyse and present their results explicitly in two ways, firstly whether the child was breastfeed at all AND secondly, if the outcomes varied depending on the differential duration of breastfeeding. Their findings of no significant benefits from breastfeeding stand in both cases, and they even note that the Obesity and BMI trends show even less of an (already a statistically insignificant) effect with regard to duration of breastfeeding.
They, as well as the second sibling study I cited, Der 2006 which ALSO analysed duration of breastfeeding, and the wealth of research from the PROBIT trial, clearly demonstrate that socioeconomic factors explain the majority of the findings in studies which fail to appropriately take these factors into account. Socioeconomic factors also likely correlate with breastfeeding duration, being a confounder in any study, no matter how well they follow the extent of breastfeeding classifications suggested in the 1990 study you mentioned, like the Raisler et a study (https://www.ncbi.nlm.nih.gov/pubmed/9987460) on infections within the first year. They did not incorporate sibling controls or any randomization methods (which is difficult), which then is a clear and potentially decisive weakness in that study. The one thing they find which *is* confirmed also by the PROBIT trial is the increased risk of diarrheal diseases in the absence of breastfeeding, and this one has the clearest suggested mechanism of action, too: the antibodies from milk present in the digestive tract itself are sufficient to help ward off an infection.
However, PROBIT did not find the changed risk to be very large in a clinical sense – as I said, no basis to ostracize the mother’s choice over – no war. I love that you say that. We should treat each other kindly no matter the feeding choice.
What comes to other effects on the mother’s health than those pointed out in the AAP overview, I would like to see reviews to confirm the effects, and if I do find such reviews that agree, I am happy to add those to the piece alongside the others listed.
Impact on ecology about producing formula? Well, that does sound like an interesting comparison to make, but just to start off, cows milk can be produced with less human inedible feed ratio than meat (cows can use fibrous human inedible plant parts for food – in fact they use significantly less human edible material compared to the amount of milk they produce), and humans often use meat as an energy source, which already suggests that the energy required to produce your average human milk may well be much higher than that of cows milk. This however is a very marginal issue compared to the fact of say, driving, or flying, or eating too much, or food waste, or… a whole army of factors that do have a great impact on the environment. I have written quite a lot about the environmental issues in my Environment and Energy sections here on the same blog, if you are interested. Those topics are very important to me.
I completely agree about the big problem with supporting women in the society, I come from the Nordics, where paid maternity leave is 16 months! There’s also subsidised child care, you name it. I do believe we should have all these things in place as well as the choice to breastfeed or bottle feed, and we should not cause unnecessary guilt or introduce needless risks for newborns in an attempt to fanatically avoid formula.
I welcome your feedback, and I am very happy that you write in a friendly and respectful manner. I am open for any other pointers you might have. But it is important to strive to talk about the details of the studies as accurately as possible, and also to consider them in their appropriate contexts – the studies with the most robust methodologies being most important, and then weighing their evidence together.
Thanks for your interest in my blog. Have a great day!
Best regards,
Iida/Thoughtscapism
LikeLike
It’s gotten to the point that some people refuse to look at evidence anymore. Why can’t people choose what’s best for them and what they feel is best for their baby?
LikeLike